
Teaching clinical reasoning using think-aloud protocols
Making the invisible visible
by Hanting Wu, PharmD, PGY1 Pharmacy Practice Resident, Magnolia Regional Health Center
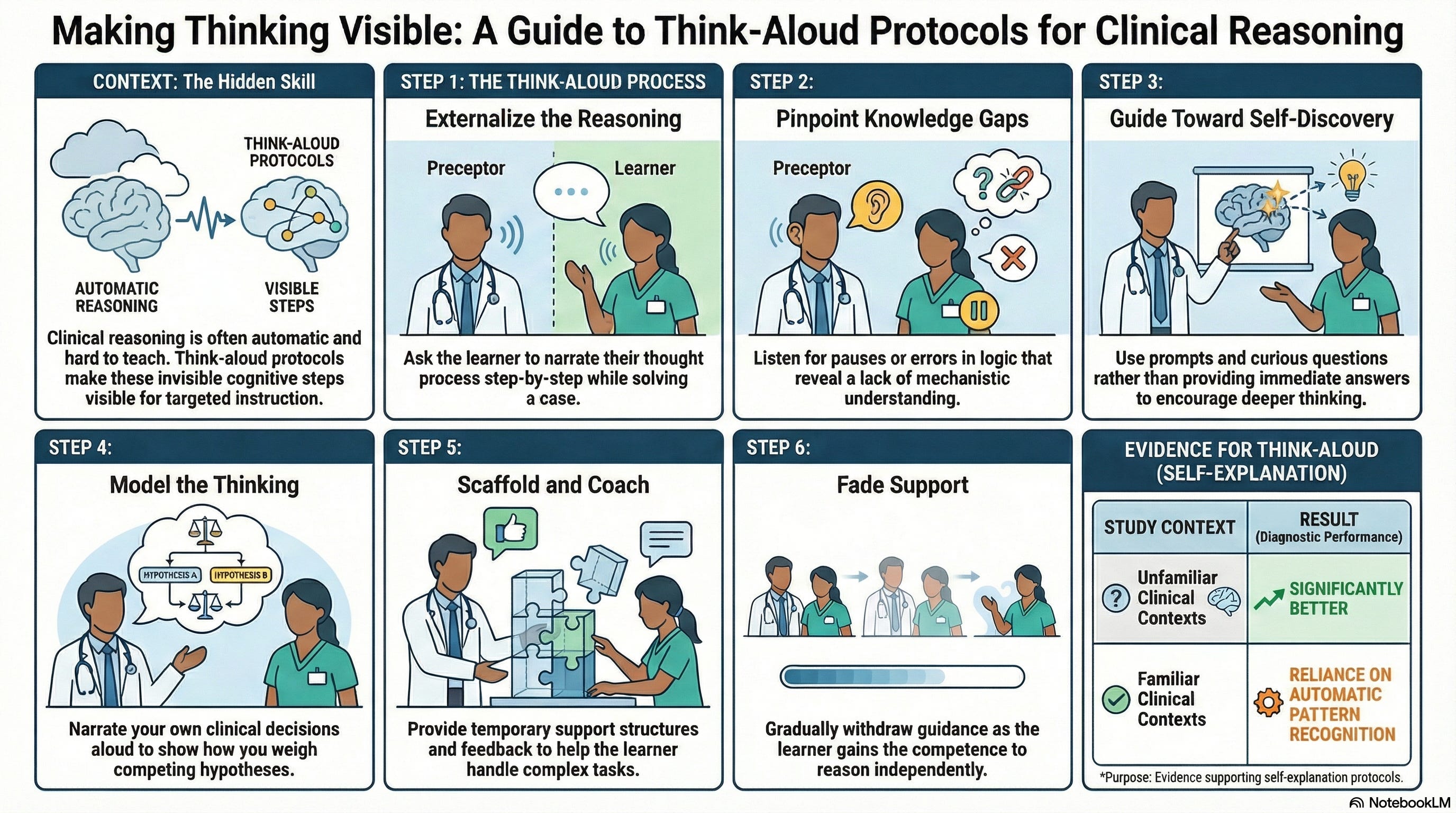
Health professional students and residents need to develop their clinical reasoning skills. However, effectively teaching this skill is challenging, as clinical reasoning requires complex cognitive processes that preceptors perform effortlessly but often don’t articulate explicitly. Think-aloud protocols offer a powerful instructional strategy to bridge this gap by externalizing the reasoning process, making the invisible cognitive steps visible, and enabling targeted correction of misconceptions or misunderstandings.

Think-aloud protocols are instructional methods in which learners or experts verbalize their thought processes as they solve problems or perform tasks. A recent experience during my internal medicine rotation exemplified their effectiveness. When co-precepting a fourth-year pharmacy student with my preceptor, we identified a concerning medication regimen: a patient was receiving both glipizide and insulin concurrently for diabetes management, despite blood glucose levels consistently maintained around 80 mg/dL—below the inpatient target of 100–180 mg/dL. I asked the student to walk through her clinical reasoning using a think-aloud approach. She began verbalizing: “Both glipizide and insulin lower blood glucose. The glucose is already at 80, below the goal. So I think the combination is a problem because both act on glucose.” I then asked her to continue thinking aloud about the mechanism of each drug. She paused and reasoned: “Insulin directly lowers blood glucose... and glipizide—it also lowers glucose, but I’m not sure exactly how it works.” This verbalized pause exposed a gap in mechanistic understanding that might have gone undetected through simple questioning. I prompted: “Keep going—what organ does glipizide target?” She continued aloud: “It acts on the pancreas, which means it stimulates the pancreas to release insulin. Oh—so glipizide is inducing endogenous insulin, which duplicates the exogenous insulin. That is why the combination creates an additive hypoglycemic effect and becomes dangerous at a glucose of 80.” By narrating each step, the student and I could pinpoint precisely where her understanding was incomplete, allowing me to provide targeted guidance rather than simply correcting her.
This example illustrates why think-aloud protocols are invaluable in clinical education. By externalizing the reasoning process, the student moved from surface-level pattern recognition to a deeper mechanistic understanding. The protocol allowed me to guide her toward self-discovery rather than simply providing an answer. This approach not only corrected a specific knowledge deficit but also modeled the systematic reasoning process, which is a skill far more durable than memorized facts alone.
This pedagogical approach aligns with cognitive learning theory, particularly the principles of cognitive apprenticeship described by Collins, Brown, and Newman2 in their seminal work on situated learning. Unlike traditional apprenticeship, which relies on observation and physical imitation of craft skills, cognitive apprenticeship makes abstract thinking processes explicit and teachable. It operates through four interconnected elements: modeling, coaching, scaffolding, and fading.
Modeling involves the expert performing a task while narrating their reasoning aloud, so learners can observe both the actions and the cognitive processes behind them. Coaching involves the instructor observing the learner’s practice, asking questions, offering targeted feedback, hints, and redirection. Scaffolding refers to the temporary support structures an instructor provides to help learners accomplish tasks beyond their current independent capability. Finally, fading involves the instructor progressively withdrawing that support as the learner gains competence and confidence. Think-aloud protocols naturally incorporate all four elements, making them a powerful vehicle for cognitive apprenticeship in clinical settings.
Empirical research supports the effectiveness of think-aloud protocols in developing clinical reasoning skills. Researchers at the Faculty of Medicine and Health Sciences, University of Sherbrooke in Quebec conducted a randomized experimental study with 36 third-year medical students to examine whether generating self-explanations improves diagnostic reasoning.1 Students were randomly assigned to a self-explanation group, verbalizing their reasoning aloud step by step while working through clinical cases during a structured training session, or a control group, who studied the same cases without the self-explanation requirement. Diagnostic performance was assessed one week later using case-based tests evaluated by raters blinded to group assignment, covering both familiar and unfamiliar clinical presentations. Students in the self-explanation group demonstrated significantly better diagnostic performance compared to controls, but critically, this benefit emerged for less familiar clinical contexts (F₁,₃₄ = 6.18, p < 0.05). This finding underscores that self-explanation is most valuable when learners cannot rely on automatic pattern recognition.
Unfortunately, expert clinicians rely heavily on automatic, intuitive cognitive processes that operate unconsciously.3 Thus, expertise creates a pedagogical challenge because experts perform complex reasoning effortlessly but struggle to teach it explicitly because they are not naturally aware of their own cognitive processes. The synthesis of cognitive science and medical education literature demonstrates that clinical reasoning can be effectively taught only when educators deliberately make their thinking visible to learners. By verbalizing how they distinguish relevant from irrelevant findings, weigh competing hypotheses, and revise their thinking based on new information, preceptors externalize the otherwise invisible reasoning processes that characterize expertise. This explicit modeling helps learners understand that expert reasoning is not linear or infallible; rather, experts entertain multiple hypotheses simultaneously, acknowledge uncertainty, and remain flexible in their therapeutic approach.
Clinical reasoning develops through deliberate practice and is accelerated when learners’ thinking becomes visible to educators. The think-aloud protocol transforms teaching from guessing at hidden misconceptions to directly addressing observable reasoning errors, showing that learners benefit most when actively verbalizing reasoning and receiving immediate feedback, creating opportunities for preceptors to model expert reasoning in direct response to specific misconceptions.
One of the biggest challenges in implementing think-aloud protocols is how to create a psychologically safe environment where learners feel comfortable externalizing imperfect or incomplete reasoning. Several practical strategies can help. First, preceptors should model the technique themselves by thinking aloud during their own clinical decision-making. For example, when a preceptor narrates uncertainty by saying: “I’m noticing the elevated creatinine, so I’m checking whether this drug is renally cleared—and whether it might need dosing adjustment...”, this normalizes iterative, sometimes imperfect reasoning and reduces learners’ fear of being wrong. Another strategy is that preceptors can respond to learner verbalizations with curiosity rather than immediate correction. This strategy sustains the think-aloud dialogue and encourages learners to reveal the full depth of their reasoning. By deliberately practicing these facilitation skills, preceptors can transform the think-aloud protocol from a theoretical concept into a powerful learning experience.
Reference
Chamberland M, St-Onge C, Setrakian J, et al. The influence of medical students’ self-explanations on diagnostic performance. Med Educ. 2011;45(7):688-695. doi:10.1111/j.1365-2923.2011.03933.x
Collins A, Brown JS, Newman SE. Cognitive apprenticeship: Teaching the crafts of reading, writing, and mathematics. In: Resnick LB, ed. Knowing, Learning, and Instruction: Essays in Honor of Robert Glaser. Erlbaum; 1989:453-494.
Pinnock R, Welch P. Learning clinical reasoning. J Paediatr Child Health. 2014;50(4):261-263.